A 48 years old male toddy tree climber by occupation since past 30 years.The Patient came with C/o chest pain since one day.C/o fever, cold and cough since 3 - 4 days.
48 years old male toddy tree climber by occupation since past 30 years,
Pt came with C/o chest pain since one day.
C/o fever, cold and cough since 3 - 4 days.
HOPI :
Pt was apparently asymptomatic 4 days back then developed fever - high grade associated with chills and rigor , on and off , relieves with medication.
C/o dry cough , aggrevates at night
C/o SOB due to excessive coughing, orthopnea - , PND -
C/o 1 episode of vomiting associated with food particles 1 day back - non bilious
Pt had similar complaints of fever associated chills and rigor in the past since 5 years
4 years back pt got hospitalized with fever and chills and got diagnosed with DM , on OHA ( met formin hydrogenchloride po/od ) - irregular medication.
In past 5 years , pt had 5 - 6 hospital admissions with similar complaints due to heavy drinking and got diagnosed with fatty liver and jaundice.
H/o seizures since 5 years
4 - 5 episodes in last 5 years , with gap of 1 year in between the episodes .
Last episode - 1 year back
Tongue bite + , Remains in unconscious state for 5 mins
H/o multiple RTA s with minor injuries over left hand, left knee, right eye, right ankle
H/o covid + 1 year back
Received 1 dose of vaccine - covishield
PAST HISTORY:
Not a /K/C/O HTN, TB , CAD, ASTHMA
No c/o abdominal pain , nausea , burning micturition
PERSONAL HISTORY : Appetite - normal
Bowel movements - Regular
Chronic alcoholic since past 30 years
Heavy drinking since past 10 years ( 360 - 480 ml/day )
Pt went to rehabilitation for 1 year ,but never stopped drinking, as told by patient attenders
O/E : Patient is C/C/C
Pallor - absent
Icterus - present
Cyanosis - absent
Edema of feet - absent
Lymphadenopathy - absent
Clubbing - absent
VITALS :
Temp : Afebrile
PR : 92
BP : 120/80 mmhg
RR : 22
SPO2 : 88 % at RA
SYSTEMIC EXAMINATION :
CARDIOVASCULAR SYSTEM :
S1 and S2 heard, no murmurs heard
RESPIRATORY SYSTEM :
Bilateral air entry present , reduced breath sounds in left IAA , IMA, ISA , on auscultation wheeze - present
CNS : NAD
PA : soft, non tender
FAMILY HISTORY: Not significant



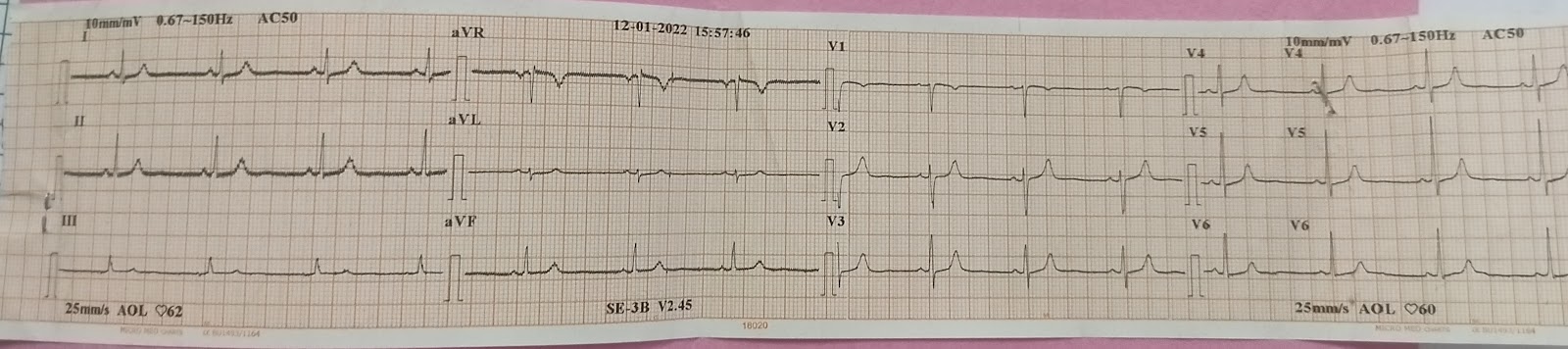
INVESTIGATIONS :

















Diabetic ketosis secondary to sepsis
Irregular medication
With Left Lower lobe consolidation
With cholelithiasis
With DM since 4 years
TREATMENT:
1. Inj PAN 80 mg/iv/stat
2. Inj. Zofer 4 mg/iv/stat
3. Inj. HAI 1 ml in 39 ml NS iv/according to grbs
4. Inj. PAN 40 mg/iv/bd
5. Inj. Zofer 4mg /iv/tid
6. Inj. Augmentin 1.2gm /iv/tid
7. Tab. Azithro 500 mg po/od
8. Inj. Thiamine in 100 ml NS/iv/tid
9. Inj. Optineuron 1 amp in 100 ml NS/iv/od
10. IVF NS, RL @ 100 ml/hr
11 Hourly GRBS charting.
Day 2
S : Chest pain reduced
1 episode of fever spike
C/o cough
On examination :
No pallor/cyanosis/generalized lymphadenopathy
Temp : 100.1
PR : 101 bpm
RR : 19 cpm
BP : 160/90 mmhg
Spo2 : 87 % at RA
CVS : S1 S2 + , No murmurs
RS : BAE + , Reduced breath sounds in left lower lobe
PA : Soft, non tender
GRBS :
8 AM : 263 mg/dl
10 AM : 154 mg/dl
2 PM : 189 mg/dl
4 PM : 194 mg/dl
8 PM : 187 mg/dl
10 PM : 179 mg/dl
2 AM : 155 mg/dl
8 AM : 178 mg/dl
A :
Diabetic ketosis secondary to ? sepsis
? Irregular medication
With ? Left Lower lobe consolidation
With cholelithiasis
With DM since 4 years
P :
1. Inj PAN 80 mg/iv/stat
2. Inj. Zofer 4 mg/iv/stat
3. Inj. HAI 1 ml in 39 ml NS iv/according to grbs
4. Inj. PAN 40 mg/iv/bd
5. Inj. Zofer 4mg /iv/tid
6. Inj. Augmentin 1.2gm /iv/tid
7. Tab. Azithro 500 mg po/od
8. Inj. Thiamine in 100 ml NS/iv/tid
9. Inj. Optineuron 1 amp in 100 ml NS/iv/od
10. IVF NS, RL @ 100 ml/hr
11 Hourly GRBS charting.
DAY 3
S : Pain reduced by 70% since admission
No fever spike
Cough reduced
On examination :
No pallor/cyanosis/generalized lymphadenopathy
Temp : 98.6
PR : 80 bpm
RR : 21 cpm
BP : 110/70 mmhg
Spo2 : 90 % at RA
CVS : S1 S2 + , No murmurs
RS : BAE +
PA : Soft, non tender
GRBS :
8 PM : 161 mg/dl
8 AM : 195 mg/dl
A :
Diabetic ketosis secondary to ? sepsis
? Irregular medication
With ? Left Lower lobe consolidation
With cholelithiasis
With GB sludge
With DM since 4 years
With Alcohol dependence
P :
1. Normal diet
2. IVF NS , RL @ 75 ml/hr
3. 8 am 2 pm 8pm
Inj. HAI 6 U - 6 U
NPH 6 U 6 U 6 U
4. Inj. PAN 40 mg/iv/bd
5. Inj. Zofer 4mg /iv/tid
6. Inj. Augmentin 1.2gm /iv/tid
7. Tab. Azithro 500 mg po/od
8. Inj. Thiamine in 100 ml NS/iv/tid
9. Syp. Benadryl 5ml PO/TID
10. Inj. PCM 1g /iv/sos
11 Hourly GRBS charting.
12. Syp. Cremaffin 30 ml/po/HS
13. Inj. KCL 2 amp in 500 ml /HS/IV over 5 hrs